
What Causes Health?
Some 95% of the trillions of dollars the US spends on health care goes to direct medical services and just 5% to population-wide approaches to prevention and health improvement. How well does that investment align with what we know about the true determinants of health?
When we think of health and longevity, we often envision doctors and nurses ministering to ill people. And yet, throughout human evolution and history, human health has improved not as much by what happens to us when we fall ill, but that we tend not to get ill. And we tend not to get ill because of safer environments (sanitation and clean water), better nutrition, and the inherent healing and self-regulatory capacities of the human organism. That is, the major determinants of human health in both developed and developing worlds are the environment (physical and social), human behavior, and our genetics—and to a lesser extent medical care.
Life expectancy in most areas of the world is increasing with the exceptions being due largely to war, epidemics, and social displacement. The improvements in life expectancy are still largely due to public health and preventive interventions (some delivered through medical care) rather than medical care provided to the already ill.
It is striking how little medical care contributed to life expectancy during the full span of the 20th century. Between 1950 and 2000 (years that coincided with the explosion in medical technology in the United States), life expectancy increased by 8.8 years; however, it increased by 20.9 years from 1900 to 1950, years when medicine often had little to offer in the way of meaningful interventions. Most of the decline in death rates for the infectious diseases that were the principal causes of death during this period occurred before a treatment or vaccine for these diseases had been discovered. A rising standard of living and the associated improvements in housing, sanitation, and nutrition account for many times more years added to our life expectancy than do all aspects of medical care combined.
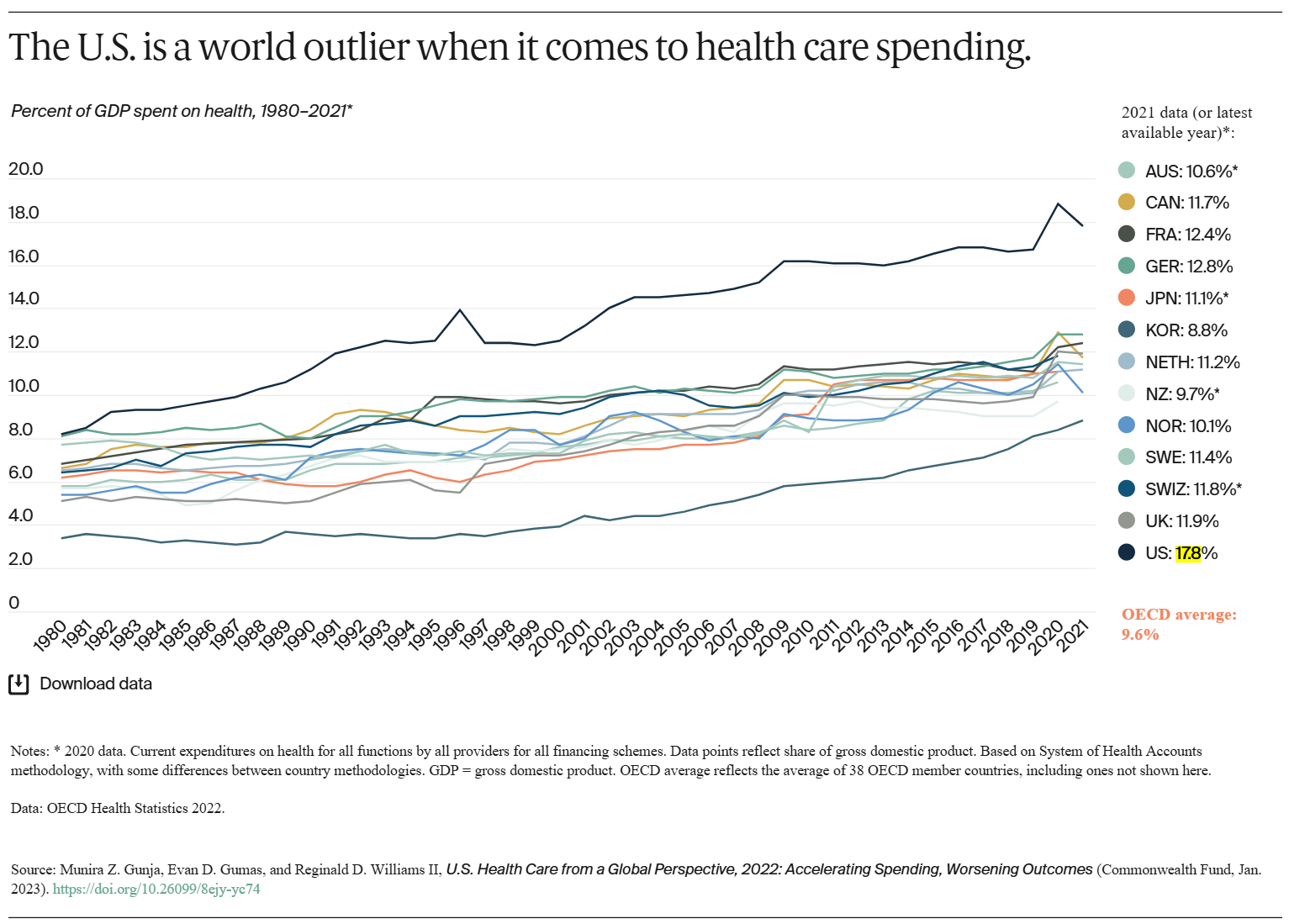
Improvements in the quality or use of medical care have a relatively limited ability to reduce deaths among Americans. This is quite surprising, given the fact that we spend 17.8 percent of our gross domestic product (GDP) on medical care. This is nearly twice the average expenditures in other developed countries. Yet, the US lags behind these countries in life expectancy. Over the course of the twentieth century, about five of the thirty years of increased life expectancy could be attributable to better medical care. The relative contribution of medical care to life expectancy rose during the latter part of the century and will likely continue to grow as technology is better able to address the health care needs of our aging population.
The benefits of medical care also come with costs: both financial and health. Medical errors, misdiagnoses, hospital-acquired infections, adverse effects and addiction to prescribed drugs, etc. all take their toll on health. In the US, medical errors alone may account for 44,000–98,000 deaths annually, or about 2–4 percent of all deaths. The Centers for Disease Control and Prevention (CDC) estimates the contribution of health care system deficiencies to total mortality at about 10 percent. According to the World Health Organization (WHO), around 1 in every 10 patients is harmed in health care and more than 3 million deaths occur annually due to unsafe care. In low-to-middle income countries, as many as 4 in 100 people die from unsafe care. Common adverse events that may result in avoidable patient harm are medication errors, unsafe surgical procedures, health care-associated infections, diagnostic errors, patient falls, pressure ulcers, patient misidentification, unsafe blood transfusion and blood clots.
The causes of death and disability can be viewed in terms of heart disease, stroke, cancer, infections, accidents, etc. But when the underlying causes of these types of disease are analyzed, a different picture emerges. On a population basis, using the best available estimates, the impacts of various domains on early deaths in the United States distribute roughly as follows:
- Genetic predispositions: 30%
- Social circumstances: 15%
- Environmental exposures: 5%
- Behavior and lifestyle: 40%
- Medical care: 10%
But more important than the proportions is the interaction of each of these domains. Whether a gene is expressed can be determined by environmental exposures or behavioral patterns. The nature and consequences of behavioral choices are affected by our social circumstances. Our genetic predispositions affect the health care we need, and our social circumstances affect the health care we receive.
Given this view, how well do our investments in health reflect the true determinants of health? In the US, approximately 95 percent of the trillions of dollars we spend as a nation on health goes to direct medical care services, while just 5 percent is allocated to population-wide approaches to prevention and health improvement. However, some 40 percent of deaths are caused by behavior patterns that could be modified by preventive interventions. In developed countries, smoking, lack of physical activity, poor diet and excessive alcohol consumption are the major contributors to death. It appears, in fact, that a much smaller proportion of preventable mortality in the United States, perhaps 10–15 percent, could be avoided by better availability or quality of medical care. Thus, one could question a funding reality that places so much emphasis on medical care and not on prevention.
Of course, longevity is not the whole picture of health. As people live longer, the number of years the average person lives with disability has increased. The major causes of years lived with disability in the US were major depressive disorder, anxiety disorder, low back and neck pain, and other musculoskeletal disorders. Medical care can sometimes markedly help people manage such disorders, such as the striking improvement of quality of life that can follow a successful hip replacement. Nonetheless, the major opportunities for improving quality of life and functioning again point to modifying diet, increasing physical activity, avoiding tobacco and excessive alcohol, as well as managing stress. And in developing countries, clean water, better nutrition, and immunizations continue to be major determinants of health.
This is not to say that medical care is irrelevant. In fact, many lives are saved or at least enriched by the careful application of medical science: from medications to surgery. Rather, we overestimate the impact of medical care on human health, and many people suffer from misuse or overtreatment as well as the lack of access to effective, evidence-based medical care.
Digging Deeper: Social Determinants of Health
“Why is Jason in the hospital? Because he has a bad infection in his leg.
But why does he have an infection? Because he has a cut on his leg and it got infected.
But why does he have a cut on his leg? Because he was playing in the junk yard next to his apartment building and there was some sharp, jagged steel there that he fell on.
But why was he playing in a junk yard? Because his neighborhood is kind of run down. A lot of kids play there and there is no one to supervise them.
But why does he live in that neighborhood? Because his parents can’t afford a nicer place to live.
But why can’t his parents afford a nicer place to live? Because his Dad is unemployed and his Mom is sick.
But why is his Dad unemployed? Because he doesn’t have much education and he can’t find a job.
But why …?”
from Toward a Healthy Future: Second Report on the Health of Canadians
While individual lifestyle choices and behavior play a significant role in health, social factors often underlie these individual behaviors and determine health outcomes. Using estimates on social determinants of health and the year 2000 mortality data, the “actual” causes of death look like this:
- Low education: 245,000
- Racial segregation: 176,000
- Poverty: 172,000
- Low social support: 162,000
- Income inequality: 119,000
These mortality estimates are comparable to deaths from the leading common diseases and injuries. For example, the number of deaths attributable to low education is comparable to the number caused by heart attacks, the leading cause of death in the United States. The number of deaths attributable to racial segregation is comparable to the number from stroke and low social support is comparable to deaths from lung cancer.
Other studies have estimated attributable fractions for mortality of 2% to 6% for poverty (depending on the year and data source), 9% to 25% for income inequality (depending on age group), and 18% to 25% for low neighborhood socioeconomic status (depending on gender and racial/ethnic group).
Low education level may even be as risky as smoking. A 2015 study estimated that 145,243 deaths in 2010 in the US were attributable to people having less than a high school diploma. To put the finding in perspective, that is comparable to the estimated number of deaths that could be averted if all current smokers had the mortality rates of people who once smoked but have stopped. Unfortunately, educational disparities appear to be widening. While life expectancy has gone up for those with higher levels of education, such as a bachelor’s degree, it has stagnated for people with less than a high school education and actually declined among women without a high school diploma.
Relative social status itself is also linked to health. A major British study of civil service employees found that, for most major categories of disease (cancer, coronary heart disease, stroke, etc.), health increased with job rank. This was true even when risk factors such as smoking, which are known to vary with social class, were taken into account. All the people in the study worked in desk jobs, and all had a good standard of living and job security, so this was not an effect that could be explained by physical risk, poverty or material deprivation. Health increased at each step up the job hierarchy. For example, those one step down from the top (doctors, lawyers, etc.) had heart disease rates four times higher than those at the top (those at levels comparable to deputy ministers). So we must conclude that something related to higher income, social position and hierarchy provides a buffer or defense against disease, or that something about lower income and status undermines defenses.
Such findings strongly suggest that strategic investments in education, reducing poverty and income equality, and improving social relations might yield considerably greater returns than continuing to escalate investments in medical care.
External Stories and Videos

More than Half Your Body is Not Human
James Gallagher, BBC
Human cells make up only 43% of the body’s total cell count. The rest are microscopic colonists. Understanding this hidden half of ourselves – our microbiome – is rapidly transforming understanding of diseases from allergy to Parkinson’s.
The Status Syndrome
How Social Standing Affects Our Health and Longevity
Michael Marmot
In this seminal study, the renowned British epidemiologist Michael Marmot shows that the lower in a socioeconomic hierarchy a person is ranked, the worse is that person’s health—a maxim that holds for almost any disease or health risk factor. Those who stand higher up on the ladder of life are always healthier than those even a few steps below. It’s not poverty that makes the difference, says Marmot, but inequality—where one stands in the hierarchy.